COLD STRESS TEST FOR HANDS E.F.J. RING
Royal National Hospital for Rheumatic Diseases, Bath UK
Summary
In 1862, Maurice Raynaud published a description of a syndrome and its symptoms. He described episodal white or bluish colouring of the extremities caused by cold. In 1970, Cosh and Ring reported on the thermographic evidence of Raynaud's phenomenon, and in 1976 a method for expressing the temperature difference between the dorsal hand and fingers after cold stress was published. Quantitative thermal imaging provided the means to apply a standardised cold challenge to the hand and measure the response to the sympathetic nervous system shown by vasodilatation and thermal recovery. Normal subjects recover from a standard exposure to water, and may produce reactive hyperaemia in the fingers. In Raynaud’s Phenomenon, there is a negative temperature gradient from wrist to finger tips, which becomes even more negative after cold stress.
A number of investigators have used different temperature water baths for this test. In our procedure 20' C is used for 1 minute, since colder temperatures can lead to extended recovery times. We determined by experiment that the critical time for recovery of the hand was 10 minutes. At this time interval normal and Raynaud patients are clearly separated. A simple index was derived to express the temperature gradient before, and after stress. On this scale values of -3 to +4,0 are regarded as normal while -4,0 to -14,0 are vasospastic, with increasing severity. In addition to the application to Raynaud’s Phenomenon, this test has proved of value in patients with Reflex Sympathetic Dystrophy (RSD). It is possible to demonstrate that an injured or painful hand does not recover in the normal way. Some of these patients have also had reduced bone mineral density measured at the radius, providing two independent and objective indications of RSD. Vibration stress to the hand has also been used to test for vibration white finger from industrial misuse. In these cases cold stress may give a normal response, while vibration applies top the finger tips induces vasospasm in these patients, which is
clearly shown by thermal imaging.
Introduction
Maurice Raynaud in 1862 described a syndrome of episodal white or bluish colour in the extremities caused by cold. It is now recognised that there are some 40 possible conditions that can lead to Raynaud's Syndrome, some of which are occupational diseases. The classification of this syndrome has been defined by a number of different groups. These often include symmetrical or bilateral involvement of the extremities, absence of occlusive lesions of the peripheral arteries, and intermittent attacks, marked by skin colour changes. A considerable number of studies have been published by investigators seeking to determine the mechanisms involved in the control of blood flow to the fingers and toes. The aetiology and pathophysiology of Raynaud's Syndrome is still not fully explained.
Techniques for monitoring blood flow are now more available, including laser Doppler flowmetry and isotope markers. Laser Doppler imaging is also available, but at present is a slow and imprecise technique. Infra red thermal imaging is a convenient non contact technique, providing dynamic two dimensional temperature measurement. By applying a standard hot or cold stress to the hand, a number of investigators have been able to monitor the temperature changes by thermal imaging (1). Skin temperature, particularly in the extremities, is highly dependent on blood perfusion. Changes in temperature are therefore representative of local blood flow. Inducing a vasospastic reaction in a patient with Raynaud's Syndrome will cause a sharp fall in temperature, and a very delayed recovery, compared with the normal reaction to the same stress.
Cold Stress Test
A technique for standardising cold stress to the hand has been used at Bath since 1976. A Standard thermogram of the dorsal surface of both hands is recorded after a 15 minute equilibration in a draught free room at 22 °c. The hands are placed on a thin board held against the chest. This provides a cool background, and enables the thermogram to be recorded with the patient sitting in a chair. At heart level, the peripheral circulation in the hands quickly stabilises.
COLD STRESS TEST
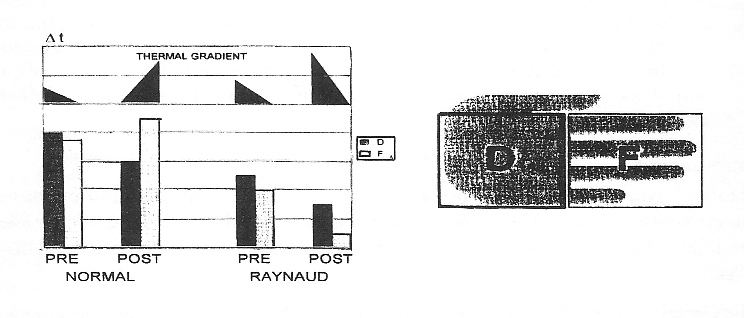
Figure 1 Vasospasticity index based on temperature gradient and the cold stress test.
The cold stress is applied by covering the hands with gloves (thin disposable plastic) and lowering into a large bowl of water at 20°c on a low trolley. The patient therefore remains seated through the whole test. 60 seconds immersion in water is sufficient to cool the hands, after which the gloves are removed, and the trolley moved away. A second thermogram is recorded 10 minutes later in the same manner as the press stress recording. The thermograms are analysed on the computer, by measuring the mean temperature of two distinct and adjacent regions of interest for each hand (Figure 1). Region one is drawn from the ulnar prominence of the wrist to the metacarpal joints. Region two is from the digital clefts to the finger tips. The mean temperatures are subtracted, 1 from 2, to express the temperature difference or gradient. Pre and post stress thermal gradients are added together to produce a simple index. In normal subjects, there is often only a slight temperature gradient from wrist to fingers before stress. 10 minutes after stress either thermal recovery has occurred, resulting in a similar gradient or reactive hyperaemia (Figure 2,). In the latter case, the fingers are hotter than the dorsal hand and a positive thermal gradient is measured. In Raynaud's Phenomenon a negative temperature gradient may exist towards the fingers before stress. This value becomes even more negative after stress. By summating both values a negative index is obtained. The more severe the condition the more negative the index. Normals can produce indices of from +4°C to -2.5°C, contrasting with values from -4° to -14° in diseased subjects ( 2,3). During the development of this test, which takes only 15 minutes to perform, many parameters were examined. Over two years, absolute hand temperatures were plotted against the external air temperatures, and a relationship was demonstrated.
Table l
Published Protocols for cold stress testing of the hand.
Temperature °C Time (mins) Author Year
0 1 Chucker 1970
0 20 (contact) Wesseling 1981
10 1 Sunawach 1982
10 1 Clark 1985
14 1 Stuttgen 1982
15 1 Bosiger 1983
16 1 Engel 1984
20 1 Ring 1980
20 1 Cooke 1982
20 1 Page Thomas 1984
20 1 Stuttgen 1984
20 1 Tauchmannova 1984
By subtracting the mean values as described, the thermal gradients were found not to correlate with external and climatic temperature. A frequent series of thermograms was also recorded following stress to plot curves of thermal recovery. The simple 10 minute reading was found to be as effective, and gave a statistically significant difference between healthy controls and known cases of Raynaud's Phenomenon. Variations in the temperature of the cold water challenge have been reported ranging from ice cold to 20°C. The less severe temperature was selected for our test, so that recovery would be achievable in the limited time available for a clinical routine test. In isolated cases, the thermogram indicates a non symmetrical response especially when individual fingers are vasospastic. These findings have usually occurred in patients with a history of industrial injury, or a known underlying pathology. The single index may not then be adequate, and individual finger temperatures are more informative. We have applied this test to 15 patients with Reflex Sympathetic Dystrophy (RSD. Sundeck's Algodystrophy). Abnormal responses have been recorded, and in many cases. where one side of the body is affected, the Index has indicated a more negative value than on the unaffected side. In vibration white finger, it is sometimes possible to record an abnormal index. However, the only effective way to indicate this disease is to apply a vibration stress, rather than a thermal stress. McHugh et al published a case report of a masonry worker who was able to produce reactive hyperaemia on cold stress testing to the hand. When a vibration plate was applied to the finger tips for 3 minutes, a marked vasoconstriction occurred, with decrease in digital temperatures (4). The frequencies required to stimulate this reaction have been variously described in the literature (1). A broadband frequency vibration from a domestic sanding tool has been found adequate for this purpose.
References
L) RingFFJ, Aarts NjM, Black CM, Bosiger P et al: Raynaud’s Phenomenon: Assessment by Tbermography (EAT Report) Tbermology 3. 69-73.1988
2.) Ring FFJ, Elvins DM. Quantification of Tbermal Images. J. Phot. Sci, ce 37. 164-167,115.1989
3.) Will RK Ring EFJ, Clarke AK Maddison Pi. Infrared Thermography, What is its place in Rheumatology in the 1990’s. Brit. J Rheumatology 31.337-344.1992
4) McHugh NJ Elvins DM, Ring EFJ. Elevated Anticardiolipin Antibodies in a patient with Vibration White-Finger, Valvular Heart Disease and Psoriatic Arthritis. Clin Rheumatology 12: 70-73, 1993.